
Claire’s MND Timeline
 While on a family summer holiday (and again in high shoes) Claire repeated the same injury
While on a family summer holiday (and again in high shoes) Claire repeated the same injury
Key Phrases Explained:
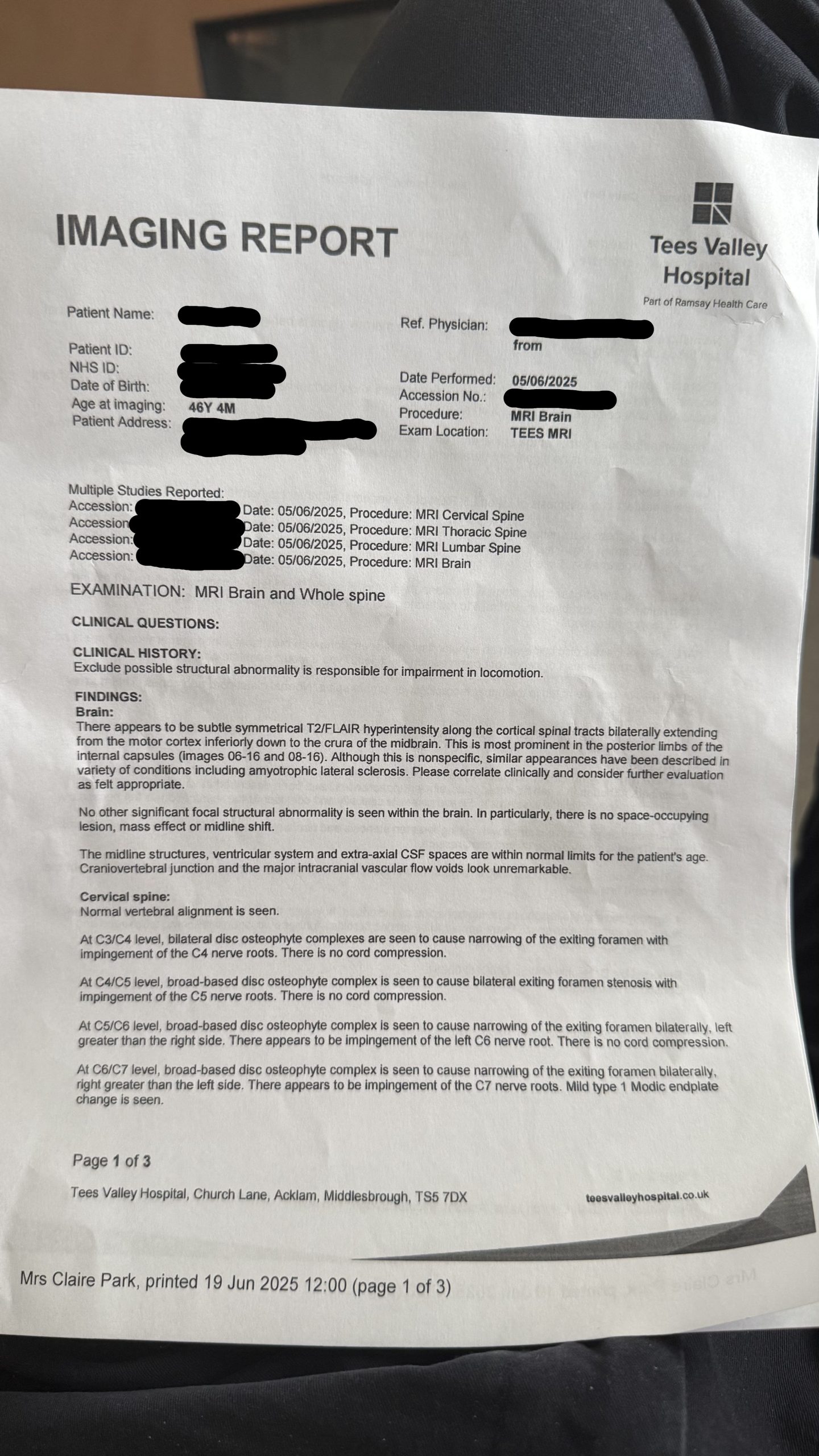
• “Subtle symmetrical T2/FLAIR hyperintensity”:
On MRI, this means there are areas in the brain that appear brighter than usual (hyperintense) on specific sequences (T2/FLAIR). These sequences are particularly good at detecting abnormalities like inflammation, demyelination, or gliosis (scarring).
• “Along the corticospinal tracts bilaterally”:
These tracts are major pathways that carry movement-related signals from the brain’s motor cortex to the spinal cord. Bilateral means it’s affecting both sides.
• “Extending from the motor cortex inferiorly down to the crura of the midbrain”:
The changes are seen starting at the motor control area of the brain and following the pathway downward through the brainstem.
• “Most prominent in the posterior limbs of the internal capsules”:
This region is a key transit point for the corticospinal tracts. It’s more affected or brighter here on the images noted.
• “Although this is nonspecific…”:
The finding is not unique to one disease. It could occur in several conditions, some of which are serious, some not.
• “Similar appearances have been described in… amyotrophic lateral sclerosis (ALS)”:
The pattern of brightness along the motor pathways can be seen in ALS, a progressive motor neuron disease. However, this is not a diagnosis, just an observation that matches patterns sometimes seen in ALS.
• “Please correlate clinically and consider further evaluation”:
The radiologist is saying: “This could be significant, but we can’t say for sure from the scan alone. The doctor should evaluate the patient’s symptoms and clinical history to decide if more testing is needed.”
⸻
Bottom Line:
This MRI shows subtle abnormalities along the brain’s motor pathways. These can be seen in conditions like ALS, but they’re not diagnostic on their own. Clinical symptoms (like muscle weakness, twitching, or stiffness) and possibly further tests (e.g., EMG, neurological exams) are needed to understand what this means for the individual.